Quick overview :
What is Vertebral sliding?
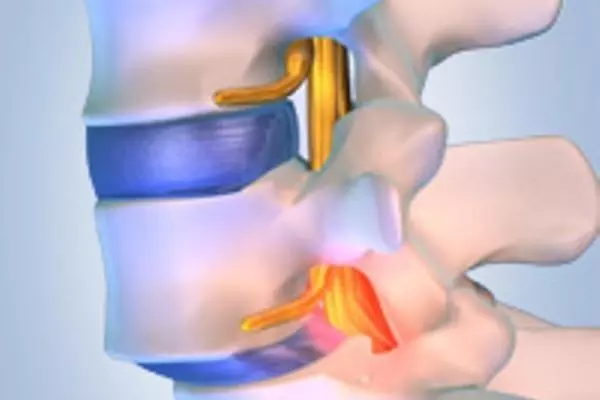
Sliding vertebrae (spondylolisthesis, retrolisthesis, olisthesis) describes a condition in which one vertebral body slides forward (spondylolisthesis) or backwards (retrolisthesis) relative to the adjacent vertebral body. Sliding back = retrolisthesis usually goes unnoticed and does not cause any symptoms. Slipping forward = spondylolisthesis can cause instability but is rare. With advanced spondyolisthesis, nerve roots can be constricted, causing back pain radiating down the leg and other characteristic neurological symptoms.
Until then, it may be that the person affected initially hardly notices that two vertebrae have become detached from the connection. Because the body often manages to compensate for the impending instability through increased muscle work. Over time, however, the constant overloading of the ligaments and muscles usually causes persistent back pain; visible changes in posture are also possible.
Common complaints
- Back pain radiating to the buttocks and/or legs
- Localized tenderness in the lower back (lumbar area)
- Numbness or signs of paralysis in one leg
- Feeling of instability in the back area
What causes slipped vertebrae? 

Vertebral slippage can be congenital (isthmic spondylolisthesis) or acquired; in the latter case, it is often caused by wear-related changes in the intervertebral space and/or vertebral joint.
In sports in which extreme backward bending of the lumbar spine is common, defects in the vertebral arch, which then result in vertebral slippage, are particularly common. However, a slipped vertebra can also develop as a result of injuries, certain bone diseases, and sometimes also as an undesirable consequence of spinal surgery.
In most cases, the slipping of the vertebrae takes place in the lumbar column area, with the penultimate (4th) lumbar vertebra very often shifting against the last (5th) lumbar vertebrae.
How is it treated?
The therapy depends on the cause of the gliding, secondary diseases, age and symptoms - we offer different therapy options here!
In the case of milder forms of vertebral slippage, it is sometimes sufficient to treat the pain with medication and to strengthen the back muscles with the help of a targeted physiotherapeutic program under professional guidance; accompanying heat treatments, electrotherapy and manual therapy can provide relief. If necessary, wearing a plaster or plastic corset bodice for several weeks can also be an option.
In younger patients with a sliding vertebra and only back pain, medical strengthening therapy is recommended first. However, if this therapy is completed without success, a stiffening operation with bone chips and - under certain circumstances - with implants such as screws can be the appropriate solution.
If a sliding vertebra causes problems that cannot be treated satisfactorily with conservative measures, or if there are neurological deficits, an operation is usually indicated. In many clinics, only one surgical option is offered for many forms of slipped vertebrae - namely the classic stiffening operation. sometimes even from the back (dorsal) and from the front (ventral) with the resulting long-lasting rebalitation time.
At the APEX SPINE Center, we offer a variety of surgical treatment options that are very individual.
- If the situation of a gliding vertebra is stable (in this case, the vertebra does not slide any further with movement of inclination / reclination) and simultaneous narrowing of the spinal canal, only the narrowing of the spinal canal is removed microscopically ( microscopic decompression ).
- In the case of an unstable gliding vertebra (here further gliding occurs in the movement function recordings) combined with a stenosis, a ligament fixation (ligament) is carried out in addition to microscopic relief . Only in very rare cases (advanced vertebral slippage> grade 2 according to Meyerding) is a spondylodesis - stiffening operation (fixation with screws and rods) indicated.
- In younger patients with a gliding vertebra without stenosis and with unilateral nerve pain, endoscopic decompression is performed in most cases
- In younger patients with a sliding vertebra and only back pain, medical strengthening therapy is recommended first. However, if this therapy is completed without success, a stiffening operation (spondylodesis) with bone chips and - under certain circumstances - without implants or screws can be the appropriate solution.