Intervertebral disc prosthesis
lumbar spine
Surgical use of a disc prosthesis
Disc degeneration can cause severe, variable, periodic back pain (with or without leg pain) that can interfere with daily life to a greater or lesser extent. Many patients with degenerative spinal disease have previously had multiple disc herniations. The degeneration is usually not visible on an X-ray image, but an MRI image clearly shows the degenerative structures.
The most important question, however, is whether the visible changes actually trigger the existing symptoms: it has been shown that patients without back pain often show significant degenerative changes, while other patients with "normal" MRI findings suffer from severe pain. In other words: imaging methods alone cannot automatically lead to a solution to the problem.
The indication for an intervertebral disc prosthesis can only be made after a precise examination and evaluation of the imaging procedures. However, if the MRI findings match the symptoms described, a solution to the problem may be within reach.
Do you have any complaints?
Then use our online questionnaire - professional initial assessment in 48 hours
 It sometimes happens that the clinical picture suggests the use of an intervertebral disc prosthesis in order to help the patient regain complete freedom from symptoms.
It sometimes happens that the clinical picture suggests the use of an intervertebral disc prosthesis in order to help the patient regain complete freedom from symptoms.
Thanks to advances in implant development, modern intervertebral disc prostheses are now optimally tailored to the special anatomical and functional conditions of the lumbar spine and therefore allow natural movement sequences, which means that the lumbar spine remains completely mobile.
They also have dampening properties similar to those found in healthy intervertebral discs. This ensures that the adjacent vertebral sections are not overloaded.
How does the treatment work?
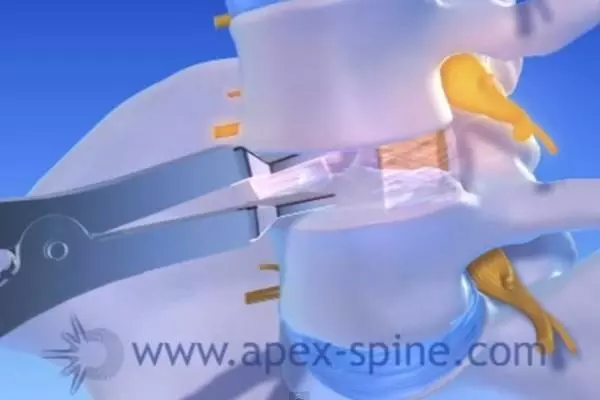
If all diagnostic findings show that a broken (degenerated) intervertebral disc is causing the symptoms, the logical consequence is the desire to replace or repair the painful intervertebral disc. The treatment principle is always the same: the intervertebral disc is removed as far as possible, whereby the important outer ring of the intervertebral disc is preserved as far as possible.
In order to prevent the vertebral height from collapsing, an artificial intervertebral disc replacement must be used in place of the diseased intervertebral disc (intervertebral disc prosthesis, cages, etc.). Due to its functionality, the intervertebral disc prosthesis appears to be a very valuable alternative for one or more painful intervertebral disc(s).
The procedure is performed under general anesthesia and takes about two hours. You can walk on your own two hours after the operation and go home on the second day after the operation.
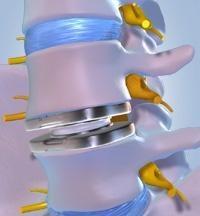
The intervertebral disc prosthesis is implanted via a small incision, usually in the lower abdomen. After removing the herniated disc, the prosthetic disc is placed between the vertebrae (intervertebral).
The replacement intervertebral disc is anchored using two titanium plates, which means that the bone can optimally grow onto the prosthesis and there is no risk of loosening. A polyethylene core lies between the two plates, and a polyurethane coating seals the prosthesis from the outside.
What aftercare is required?
As a rule, patients can leave the recovery room on their own about 2 hours after the procedure. On the first day after the operation you can eat light food. To prevent the risk of thrombosis, you will be given heparin before the procedure and until you are discharged.
You can leave the clinic after about 4 days. It is necessary to wear a soft bandage for about six weeks, after which it is advisable to start physiotherapy individually tailored to you under the supervision of a physiotherapist.
Driving or cycling are allowed once the abdominal scar has healed. If an optimal positioning of the implant has been determined after an X-ray examination, experience has shown that the implant can withstand all loads - such as fast walking, falling or jumping.
When can you do sports again?
You should be able to swim or cycle regularly again about six weeks after the procedure. You can gradually resume your usual sporting training around nine to twelve weeks after the procedure.
When are you able to work again?
After six weeks you can resume office work and light physical work. You should avoid heavy physical activity for the first twelve weeks and then slowly increase it.
What is the success rate? And what are the risks?
In the international literature, success rates of around 85 percent are given.
In the hands of an experienced surgeon with modern implants, the likelihood of complications is very low. The most common risks of intervertebral disc prosthesis surgery are: insufficient pain reduction (10-15%), residual pain from radiation (5%), deep vein thrombosis (1%), long-term facet degeneration possible (no percentage information available), incorrect positioning, sinking of the prosthesis - mostly due to insufficient bone density (women> 45 years). Pain can remain after each operation, but the likelihood of reoperation after prosthetic surgery is 50% lower than after fusion.
The number of patients who can return to work in perfect condition after surgery is much higher after prosthetic surgery than after fusion (Source: Round Tables In Spine Surgery, Volume 1 o Number 4 o 2006, B. Conix, R. Hes, Middelheim, Antwerp)
At a glance!
| The most important facts and data are summarized and compared for you at a glance | ||
|---|---|---|
| stiffening operation | intervertebral disc prosthesis | |
| risk |
|
|
| Pains |
|
|
| After the procedure |
|
|
| hospital stay |
|
|
| surgery |
|
|
| Sports |
|
|
| meeting |
|
|
!!! The mobility and functionality of the spine is preserved !!!
The advantages at a glance:
- Modern intervertebral disc prostheses ensure natural mobility and
unrestricted functionality of the damaged lumbar spine - A feared connection degeneration can usually be avoided
- Independent movement and walking possible immediately after the operation
- Speedy recovery and pain relief
- No longer hospital stay is necessary:
In general, you can go home four days after the operation. - You can largely resume your usual activities six weeks after the operation
- Short rehabilitation phase and quick return to work (4 - 6 weeks)
- A high success rate of approx. 85%